Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Lung in Health and Disease
- General Approach to Patients
With Respiratory Disorders - Evaluating Lung Structure and Function
- Interstitial Lung Diseases
- Pulmonary Vascular Diseases
- Disorders of the Pleura,
Mediastinum, and Chest Wall - Respiratory Failure
- Lung Transplantation
- Perioperative Pulmonary Management
- COVID-19 Pulmonary Management
- Congenital Lung Malformations
- Sleep-Related Disorders
Cough
Cough, sputum production, and dyspnea are the cardinal features of respiratory diseases. One of these symptoms may prevail according to the underlying pathology, but quite often they occur concurrently. Cough and expectoration are particularly frequent in patients suffering from chronic airway diseases, such as chronic obstructive lung disease, bronchial asthma, bronchiectasis, and, in severe forms, i. e., at a certain level of functional impairment, patients complain about shortness of breath. However, in restrictive lung diseases dyspnea is often the leading complaint, whereas an unproductive cough remains a complementary symptom.
Pathophysiology
Cough is a complex reflex
initiated by the irritation of cough receptors
located in the upper and lower airways. Cough
serves as a protective mechanism against noxious
inhalants. It represents an important bronchial
clearancemechanism, indicates air pollution, and
is a cardinal symptom of various lung diseases.
In healthy persons cough is a physiologic
reaction to inhaled irritants, in sick people it
is the most common and often the first symptom
of a diseased lung. Cough may indicate impaired
mucociliary clearance, which requires an intact
respiratory epithelium and bronchial secretion
of normal rheologic properties. Viral infections
of the lower airways are the most common causes
for transiently impaired mucociliary clearance,
whereas cigarette smoking is the most common
cause for a permanently damaged clearance.
Clinical Findings
A distinction should be
made between acute and chronic, as well as
between unproductive, i. e., dry and productive
cough, i. e., cough accompanied by sputum
production.
Acute episodes of cough are
common at any age and are most often due to
viral airway infections. In this case, cough is
self-limiting and needs no further work up.
Treatment is either not necessary or only
symptomatic. Chronic cough lasts longer
then-eight weeks by definition. It is quite
often a diagnostic challenge.
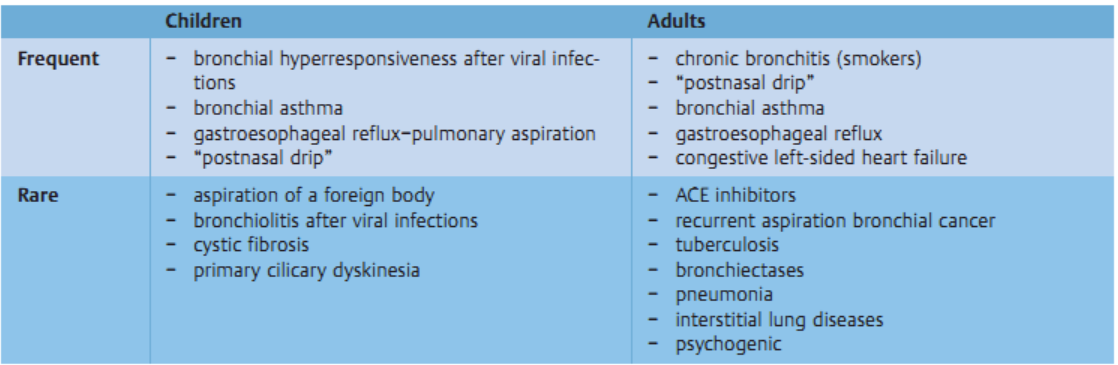
Etiology
The following diseases can cause chronic cough.
In children, cough is frequently due to
prolonged viral infections or postviral
bronchial hyperreactivity. In childhood, cough
is quite often the single symptom of asthma.
Other causes are: foreign body aspiration,
cystic fibrosis, and other lung diseases, which
lead to impaired development and growth. In
adults, the most common causes of cough are
chronic bronchitis in cigarette smokers,
bronchial asthma, chronic rhinosinusitis with
postnasal drip, and gastroesophageal reflux.
Other causes are bronchial carcinoma,
tuberculosis, and diffuse infiltrative lung
diseases. Chronic coughmay also be due to
left-sided heart failure or it is caused by
treatment with angiotensin converting enzyme
(ACE) inhibitors. In elderly people cough may be
due to recurrent aspiration or an aspirated
foreign body. Cough is rarely a leading symptom
in diseases of the pleura, the diaphragm, or the
pericardium. Rare cases have been reported in
which cough was due to an irritation of the ear
drumby hairs in the external ear channel.
Causes for chronic cough
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Pulmonary symptoms, findings and investigations
Assessment of chronic cough
Expectoration
Hemoptysis
Pleural Effusion
Approach to wheezing in children
Polysomnography
Pulmonary Function Testing
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.