Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
ABDOMINAL PAIN CHRONIC
A great deal of knowledge and
skill is required to practice as a doctor.
Physicians in the 21st century need
to have a comprehensive knowledge of
basic and clinical sciences, have
good communication skills, be able
to perform procedures, work
effectively in a team and
demonstrate professional and ethical
behavior. But how doctors think,
reason and make decisions is
arguably their most critical skill.
Knowledge is necessary, but not
sufficient on its own for good
performance and safe care.
Most abdominal pain is localized, for example
that due
to a renal stone or biliary stone,
acute appendicitis
or peptic ulceration.
There are, however, a number of
causes of
generalized abdominal pain, the most
common
of which are peritonitis and intestinal
obstructions.
A list of causes to be
considered includes:
1.
General
peritonitis
2. Tuberculous peritonitis
3.
Intestinal obstruction
4. Lead colic (rare)
5. Gastric crises (rare)
6. Abdominal angina
7.
Functional abdominal pain
8. General
medical diseases:
• Malaria
• Porphyria
• Diabetic ketosis
• Blood dyscrasias
•
Henoch's purpura
• Sickle-cell anemia
•
Hypercalcaemia
GENERAL PERITONITIS
Peritonitis must be secondary to a lesion that
enables
some clue in the history to suggest
the initiator
disease. Thus, the patient with
established peritonitis
may give a history of
onset that indicates acute
appendicitis or
salpingitis as the source of origin.
Where
the onset of peritonitis is sudden, one should
suspect an acute perforation of a hollow viscus.
The early features depend on the severity and
the
extent of the peritonitis. Pain is always
severe, and
typically the patient lies still
on his account – in contrast
with the
restlessness of a patient with abdominal colic.
An extensive peritonitis that involves the
abdomen
aspect of the diaphragm may be
accompanied by
shoulder-tip pain. Vomiting
often occurs early in the
course of the
disease. The patient is obviously ill, and
the temperature frequently elevated. If
initially the
peritoneal exudate is not
purulent, the temperature
may be normal. It
is a good aphorism concerning
the two common
causes of this condition that
peritonitis due
to appendicitis is usually accompanied
by a
temperature above 38 °C (100 °F), whereas the
temperature in peritonitis due to a perforation
of a peptic ulcer rarely reaches this level. The
pulse is
often raised and tends to increase
from hour to hour.
Examination of the abdomen
demonstrates
tenderness, which may be
localized to the affected area
or is
generalized if the peritoneal cavity is
extensive
involved. There is marked guarding,
which again may
be localized or generalized,
and rebound tenderness
is present. The
abdomen is silent on auscultation,
although
sometimes the transmitted sounds of the
heart
beat and respiration may be detected. Rectally,
there is tenderness of the pelvic peritoneum.
As the disease progresses, the abdomen becomes
distended, signs of free fluid may be detected,
and
the pulse becomes more rapid and feeble.
Vomiting is
now effortless and feculent, and
the patient, although
still conscious and
mentally alert, demonstrates the
Hippocratic
facies with sunken eyes, pale, cold and
sweating skin, and cyanosis of the extremities.
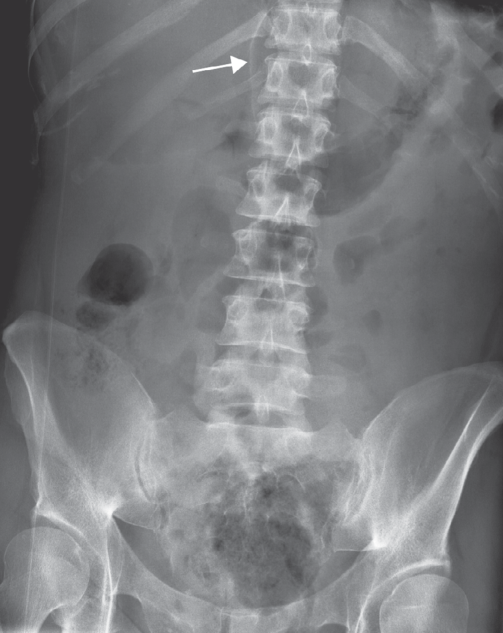
An X-ray of the abdomen in the erect position
may
reveal free subdiaphragmatic gas in
peritonitis due to
hollow viscus perforation
(e.g. perforated peptic ulcer),
but its
absence by no means excludes the diagnosis (the
photo below - abdominal radiograph showing the
falciform ligament outlined by free
intraperitoneal gas (arrowed).).
The main differential
diagnoses are the colic of
intestinal
obstruction or of ureteric or biliary stone.
Intraperitoneal haemorrhage, acute pancreatitis,
dissection or leakage of an aortic aneurysm, or
a basal
pneumonia are also important
differential diagnoses.
TUBERCULOUS
PERITONITIS
In Great Britain, this is now a
rare disease. When it
is encountered in the
UK, the patient is usually an
immigrant from
a developing country. Usually, there is
a
feeling of heaviness rather than acute pain. The
onset
of symptoms is gradual, with abdominal
distension,
the presence of fluid within the
peritoneal cavity, and
often the presence of
a puckered, thickened omentum,
which forms a
tumor lying transversely across the
middle of
the abdomen.
INTESTINAL COLIC
INTESTINAL OBSTRUCTION
This is a common cause
of generalized abdominal pain.
In
peritonitis, there is no periodic rhythm,
whereas
waves of pain interspersed with
periods of completeness
relief or only a dull
ache are typical of obstruction.
In contrast
to the patients with peritonitis who wish
to
remain completely still, the victim of
intestinal
obstruction is restless and rolls
about with the
spasms of colic. Usually,
there are the accompaniments
of progressive
abdominal distension, absolute
constipation,
progressive vomiting (which becomes
faeculent), and the presence of noisy bowel
sounds on
auscultation. An X-ray of the
abdomen usually reveals
multiple fluid levels
on the erect film, together with
distended
loops of gas-filled bowel, which are obvious
on the supine radiograph.
The presence of a
scar (or scars) of previous abdominal
surgery, performed no matter how long
previously,
strongly suggests postoperative
adhesions or bands as
the cause of the
obstruction. Careful examination of the
hernial orifices – inguinal, femoral and
umbilical – is
mandatory to diagnose a
strangulated external hernia.
Surprisingly,
the patient may be completely ignorant
of its
presence. I has seen a distinguished
anesthetist who correctly diagnosed his own
acute
bowel obstruction but had not noticed
his strangulation
inguinal hernia.
LEAD COLIC
Lead colic
may cause extremely severe attacks of
general
abdominal pain. There may be preceding
anorexia, constipation and vague abdominal
discomfort. The severe pain is usually located
in
the lower abdomen and radiates to both
groins; it
may also sometimes be associated
with wrist-drop (due to peripheral neuritis),
and occasionally with lead
encephalopathy.
There may be a blue 'lead line' on the
gums
if oral sepsis is present, due to the
precipitation
of lead sulphide. Frequently,
there is a normocytic
hypochromic anemia with
stippling of the red cells
(punctuate
basophilia). Inquiry about the patient's
occupation may well be the first clue to the
diagnosis.
GASTRIC CRISES
Gastric
crises in neurosyphilis, although rare, may
causes general abdominal pain. The patient has
other
evidence of tabes dorsalis, with Argyll
Robertson
pupils, optic atrophy and ptosis,
loss of deep sensation
(absence of pain on
testicular compression or
squeezing the
Achilles tendon), and loss of ankle and
knee
jerks. The pain is severe and lasts for many
hours
or even days. There may be accompanying
vomiting,
and there may also be rigidity of
the abdominal wall.
The crisis visceral may
be the sole manifestation of
tabs. The mere
fact that a patient has tabes dorsalis
does
not, of course, mean that their abdominal pain
must necessarily be a gastric crisis. The author
has
repaired a perforated duodenal ulcer in a
patient with
all the classic features of
well-documented tabs
dorsalis.
ABDOMINAL ANGINA
Abdominal angina occurs in elderly patients as a
result of progressive atheromatous narrowing of
the
superior mesenteric artery. Colicky
attacks of central
abdominal pain occurs
after meals, and this is followed
by
diarrhea. Complete occlusion with infarction of
the
intestine is often preceded by attacks of
this nature.
Occlusion of vessels to the
small or large intestine - as
is seen in a
number of vasculopathies such as systemic
lupus erythematosus (SLE) or polyarteritis
nodosa –
may cause generalized abdominal pain
and proceed to
gangrene, perforation and
general peritonitis.
FUNCTIONAL ABDOMINAL PAIN
One of the most difficult problems is the
patient (female
more often than male) who
presents with severe chronic
generalized
abdominal pains and in whom all clinical,
laboratory and radiological tests are negative.
Inquiry
will often reveal features of
depression or the presence
of some
precipitating factor producing an anxiety state.
In some cases, the abdomen is covered with scars
previous laparotomies at which various organs
have
been reposited, non-essential viscera
removed, and real
or imaginary adhesions
divided. Some of these patients
prove to be
drug addicts, others are frank hysterics, and
others seek the security of the hospital
environment,
but in still others the etiology
remains mysterious.
This forms one type of
the so-called 'Munchausen's'
syndrome',
described by the late Dr. Richard Asher.
ABDOMINAL PAINS IN
GENERAL DISEASE
Acute abdominal pain may
occur in a number of
medical conditions not
already considered. These
include sudden and
severe pain complicating
malignant malaria,
familial Mediterranean fever and
cholera, or
the pain may accompany uncontrolled
diabetes
with ketosis, that rare condition known
as
porphyria and any of the blood dyscrasias; the
best examples are Henoch's purpura in children
and the abdominal colic of acute sickle-cell
crisis. Bouts of abdominal pain may occur in the
hypercalcaemia of hyperparathyroidism.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Toxicological risk during pregnancy
We use the commonly known FDA classification
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.