Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
AMNESIA
Memory is the ability to store and subsequently retrieve past experience, and it is fundamental to many cognitive functions. Amnesia can be defined as a loss of previous memories and an inability to form new ones. Altered alertness, attention, language and motivation may all confound the clinical assessment of memory function, and they must be absent for the term 'amnesia' to have clinical usefulness. Memory is conventionally divided into registration (which includes perception in all modalities); encoding and storage; and retrieval. Learning includes encoding and the initial storage of information.
CLASSIFICATION AND NOMENCLATURE
Memory is
not a unitary function and can be divided up in
many different ways. One classification is
presented in the table. It is conventional to
divide memory into short-term (also called
primary, immediate or working) memory and
long-term (also called secondary) memory.
Long-term memory may be further subdivided into
recent (from initial learning to hours) and
remote (extending back to childhood). Short-term
memory is tested at the bedside by digit span
testing, although poor attention can confound
this test. A normal person's digit span is seven
or eight digits, which are forgotten over about
30 seconds unless rehearsed. Long-term memory
has been traditionally regarded as a
consolidated form of short-term information, but
this concept does not explain patients with
impaired digit span but normal
learning and
long-term memory. Ribot's law states that there
is an inverse relationship between memory
strength and recency (i.e. older memories are
better preserved), and is a useful guiding
principle often seen clinically. Semantic memory
refers to an individual's store of previously
acquired facts, concepts, words and beliefs, and
is conceptually rather similar to long-term
memory. Procedural memory is outside conscious
awareness, and it allows the patient to remember
how to perform tasks, for example driving or
cycling. It may be relatively resistant to
disease processes that profoundly affect the
recent memory system, such as Korsakoff's
syndrome or Alzheimer's disease.
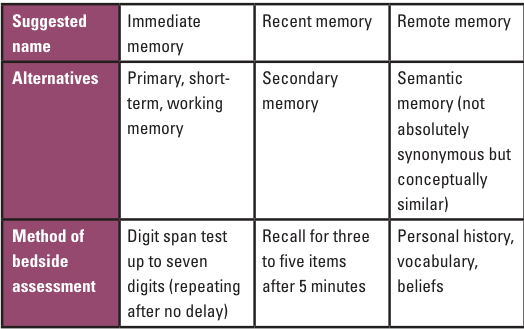
Memory nomenclature above.
FUNCTIONAL ANATOMY OF MEMORY
Functional
imaging of cerebral blood flow suggests that the
prefrontal cortex is important for tasks
involving working memory. Recent memory function
involves a pathway that includes the hippocampus
and the adjacent entorhinal cortex, which are
rich
connected to multimodal neocortical
association areas.
The hippocampus is thought
to form new associations between ordinarily
unrelated events, and damage therefore impairs
learning. Midline structures, such as the medial
and anterior thalamic nuclei and mamillary
bodies, are also critical for recent memory.
Functional imaging studies show that the
hippocampus is activated during encoding;
moreover, material that evokes the
most
parahippocampal gyral activation is most likely
to be remembered. There are anatomical links
between the hippocampal formation and the
midline structures, but the interaction between
these structures is not well understood. The
bilateral representation of the midline
structures critical for memory means that
bilateral cerebral damage is usually necessary
to produce a severe amnesic syndrome.
Functional links between the working memory
system (involving the prefrontal cortex) and
recent memory system (involving the hippocampus,
parahippocampal gyri and midline structures)
must be important in creating long-term
memories, which are likely to be stored in the
neocortex.
The cholinergic neurotransmitter
system plays a key role in recent memory, as
shown by the damage to forebrain cholinergic
projections in Alzheimer's disease. Furthermore,
cholinergic antagonist drugs, for example
scopolamine, markedly impair recent memory and
learning.
The synaptic basis for the encoding
and storage of memories is an area of active
research. The process of long-term potentiation
(the modification of a synapse's strength by the
neural traffic across it) has been the most
widely cited mechanism by which neural networks
'learn'. Memory disorders are common. When
making a diagnosis in a clinical setting, it is
useful to divide them according to whether the
onset is rapid or gradually progressive, and
whether they are of short duration or
persistent. These types of memory loss are now
considered.
RECENT MEMORY LOSS OF RAPID ONSET AND
SHORT DURATION
Transient global amnesia
This is the prototype syndrome of recent memory
loss with preserved attention. It occurs in
middle-aged and elderly patients who develop
sudden amnesia and bewilderment lasting several
hours. There is amnesia for the recent past, as
well as anterograde amnesia. They typically ask
questions about their circumstances over and
over again: 'Where am I?', 'How did I get
here?', 'What time is it?' There is no
impairment of consciousness, and the ability to
do even complex tasks (procedural memory) is
preserved. Patients remain capable of high-level
intellectual performance throughout. Normal
memory function will return within minutes to
hours, and the patient has no subsequent recall
for the period of amnesia and a brief spell
before the attack. Most patients suffer only a
single attack, but there is an annual risk of
recurrence of about 5 percent.
The cause of
this syndrome is uncertain, but antecedent
events are commonly identified, including
emotion or stress, cold water exposure, sexual
intercourse and mild head trauma. It has been
suggested that transient global amnesia (TGA) is
due to an unusual form of complex partial
seizure activity or cerebral ischaemia. Recent
data from diffusion-weighted magnetic resonance
imaging have shown restricted diffusion in the
left mesial temporal lobe in seven out of ten
patients during an attack, suggesting that TGA
may have similarities with the cortical
spreading depression thought to underlie
migrainous aura propagation. A history of
migraine is often found in patients with TGA.
In clinical practice, the important conditions
to be considered in the differential diagnosis
of TGA are complex partial seizures, and
posterior circulation ischaemia (which will
usually cause additional brainstem symptoms and
signs). Transient ischemic attacks (TIAs)
involving isolated ischemia of the thalamus or
hippocampi may produce selectively impaired
recent memory and a TGA-like syndrome.
Once
the diagnosis of TGA is secure, the patient can
be reassured that the condition is remarkably
benign, with no increased risk of ischemic
stroke.
Ictal amnesia
Amnesia for the duration of
the seizure is usual in tonic-clonic seizures,
complex partial and absence seizures, due to
disrupted electrical activity in components of
the brain memory systems. There may be brief
retrograde amnesia prior to attacks as well as a
period of post-ictal amnesia. Memory loss may
occasionally be the only symptom of an epileptic
seizure involving temporal lobe structures,
although observers usually describe speech or
motor
disturbance, or automatic behaviours.
The brief episodes of memory disturbance seen in
childhood 'petit mal' absence may cause problems
with learning and behaviour. Rarely, complex
partial seizures in adults may result in
prolonged non-convulsive status epilepticus,
which may last for days or weeks and for which
the patient is subsequently amnesic.
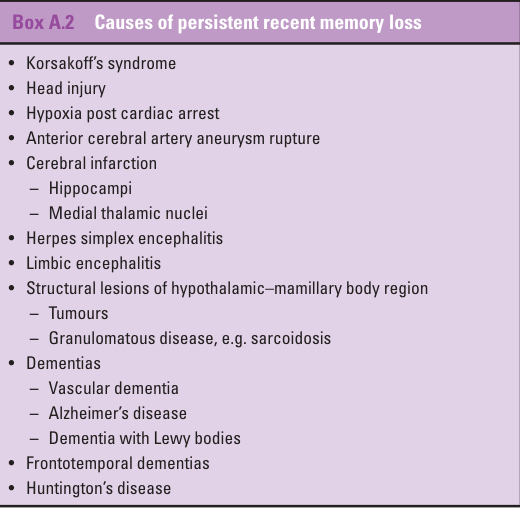
PERSISTENT RECENT MEMORY LOSS
Korsakoff's
syndrome
Korsakoff's syndrome, first
described between 1887 and 1891, is a dramatic
example of the amnesic syndrome. It is related
to thiamine deficiency and commonly associated
with long-term alcohol abuse, although it can
also result from other causes of thiamine
deficiency such as persistent vomiting
(including hyperemesis gravidarum), intestinal
obstruction, malabsorption, puerperal sepsis and
metastatic carcinoma. It usually follows or
accompanies Wernicke's encephalopathy, which is
characterized by confusion, ophthalmoplegia and
ataxia. The definition of a pure Korsakoff's
syndrome requires that the patient is awake and
attentive, responsive, and capable of
understanding language, making appropriate
deductions and solving problems. Newly presented
information is correctly registered, but cannot
be retained for more than a few minutes
(anterograde amnesia or learning failure). There
may be an associated variable dysfunction of
recall of older memories – days, weeks or even
years – i.e. retrograde amnesia. Confabulation,
or falsification of memory, is commonly (but not
invariably) seen. If recovery occurs, the period
of retrograde amnesia shrinks but leaves a gap
in memory for the period of anterograde amnesia
following the onset of the illness.
Neuropathological studies have shown a
degeneration of neurons and loss of myelin in
the mamillary bodies, the anteroventral and
pulvinar nuclei of the thalamus, and the fornix.
Head injury
A severe head injury,
sufficient to impair consciousness, invariably
results in amnesia for the period of
unconsciousness. It is also apt to cause
retrograde amnesia, which extends for seconds,
minutes or sometimes hours prior to the injury,
and post-traumatic amnesia (PTA), which extends
for days, weeks or, rarely, months after the
injury. PTA is associated with reduced
orientation and difficulty learning, and
therefore has a major impact on rehabilitation.
The duration of the retrograde amnesia will tend
to shrink with time, whereas the anterograde
amnesia is more persistent. The duration of PTA
is of considerable value in assessing the
severity of injury and prognosis: the longer the
PTA, the more severe the head injury and the
poorer the prognosis.
As a guide, of patients
with PTA of less than an hour, 95 percent can be
expected to return to work within 2 months; if
the amnesia lasts over 24 hours, only 80 percent
will return to work at 6 months. The most
severely injured may remain permanently
disabled.
Patients who have recovered
consciousness may appear capable of conversing
and carrying out normal activities, yet are
unable to recall these activities later when
recovery is complete because they are still in a
state of PTA. This can impair their
rehabilitation, and must be taken into account.
Following recovery from PTA, patients may be
forgetful and may complain of problems with
memory for 2 or 3 years. A residual defect
remaining this long is likely to be permanent.
Assessment of memory loss after head injury
is difficult, and is sometimes influenced by
litigation.
Formal psychometric assessment of
memory function should always be undertaken,
although this may be difficult or impossible in
the context of profound PTA.
Head injuries
that do not cause loss of consciousness are
unlikely to result in severe amnesia.
Penetrating wounds of the head, unless they
specifically injure the medial temporal lobes,
are also unlikely to cause problems with memory.
Permanent memory defects may follow single
severe acute head injuries or repeated minor
traumas, as in the case of boxers (dementia
pugilistica). The pathology of memory loss after
closed head injury varies. Trauma can result in
cerebral edema followed by infarction of the
hippocampus and cingulate gyri. Memory loss may
be due to diffuse microscopic injuries causing
diffuse axonal injury.
Vascular disease
Bilateral limbic
structure infarction (including the hippocampi
and medial thalamic nuclei) may cause persistent
amnesia. There are often associated neurological
signs to indicate posterior cerebral artery
territory infarction, including visual
disturbances, cortical blindness, aphasia or
alexia. Unilateral infarction in the same areas
may rarely cause problems with memory. Isolated
frontal infarcts have also been reported to
cause memory impairment. Patients who suffer
rupture of an anterior communicating artery
aneurysm, or undergo surgical treatment for such
a lesion, may suffer ischaemia (due to
vasospasm), and consequent infarction in the
distribution of the small penetrating branches
of the anterior communicating artery. This
results in damage to the posterior inferior
medial frontal areas, and to the anterior
portion of
the fornix and corpus callosum.
These patients may present with acute amnesia,
which may recover in those in whom the ischaemia
is temporary and related to vasospasm.
An
acute hypoxic cerebral insult, such as that
resulting from cardiac or respiratory arrest, or
after carbon monoxide poisoning, may produce an
irreversible amnesic syndrome because of
involvement of the medial temporal lobes and
thalamus.
Encephalitis and other inflammatory
conditions
Herpes simplex encephalitis is a
striking cause of an acute persistent amnesic
syndrome. Patients with this severe illness
typically present with seizures, behavioral
changes, encephalopathy, dysphasia and
hemiparesis; because of the predilection of the
virus to cause haemorrhagic infarction in the
temporal lobes, there may be a specific amnesic
syndrome.
If memory deficits persist for 1
month or more, the prognosis for recovery is
likely to be poor. In addition to herpes simplex
infection, any pathological process involving
the functional networks underlying memory
systems, particularly limbic structures, can
cause amnesia. Subtle cognitive decline
frequently
occurs in multiple sclerosis and,
in rare cases, there may be specific and severe
memory impairment.
Neurosarcoidosis, cerebral
lupus and neurological Behçet's disease may also
cause memory impairment.
In patients with
small-cell lung carcinoma, there is an
associated form of 'limbic encephalitis' in
which memory defects occur as a non-metastatic,
distant manifestation of the cancer. Specific
antibodies to neuronal components (most commonly
anti-
Hu antibodies) may be identified in
serum or cerebrospinal fluid. More rarely, this
syndrome can be associated with other tumors,
including carcinoma of the testis or breast.
Cerebral tumor
Amnesic syndromes are rare as
the presentation of cerebral tumors. They do
nevertheless occur with masses arising in the
diencephalus–mammary body region in the midline.
Causes include corpus callosum tumors (e.g.
astrocytoma) arising in the region of the
fornix. The fornix may be damaged after removal
of a
colloid cyst of the third ventricle,
causing postoperative
amnesia.
Memory loss associated with dementias
Insidious recent memory loss is the most common
presenting symptom in Alzheimer's disease, and
it becomes increasingly severe as the condition
progresses. Other neurodegenerative conditions,
including the frontotemporal dementias, may also
involve memory function, although recent memory
is typically preserved for longer in these
illnesses than in Alzheimer's disease. Dementia
with Lewy bodies, progressive supranuclear palsy
and corticobasal degeneration may all involve
progressive recent memory impairment, but these
should have other neurological features to
suggest the correct diagnosis. Vascular dementia
is another common cause of progressive
(classically 'stepwise') memory impairment, and
infarctions in the thalamus
or hippocampi, or
in the white matter pathways connecting these
regions to the neocortex, are the probable
cause. In all of these conditions, the
progression of memory loss is usually associated
with intellectual, perceptual, linguistic,
praxic, attentional, personality and mood
disturbances, indicating the diffuse evolving
nature of the underlying pathology
OTHER TYPES OF MEMORY LOSS
Drugs
Many
drugs impair memory as part of a central nervous
depressant effect, but others have a more
specific amnesic effect. The latter include
cannabis, organic solvents, heavy metals such as
lead and mercury, anticonvulsant drugs,
anticholinergic drugs
and benzodiazepines.
Older anticonvulsant drugs, particularly
phenytoin and the barbiturates, have marked
effects on memory in normal volunteers and in
patients with epilepsy. The new anticonvulsant
topiramate may also cause mental slowness and
verbal learning disturbance. Other new
anticonvulsant drugs, including gabapentin and
lamotrigine, appear to have fewer cognitive side
effects than older medications.
'Psychogenic
amnesia'
Complaints of memory impairment are
common in depression and anxiety, but formal
assessment with psychometry will usually reveal
that reduced attention motivation or low mood is
the cause for the symptom. More florid
psychogenic amnesic states do
occur, but
differ from organic amnesia in the pattern of
the memory defect and in the time course of
onset and recovery. Loss of personal identity is
common in psychogenic amnesia, but extremely
rare in organic amnesia. The common setting of
the 'psychogenic fugue', in which the patient is
discovered wandering,
often a long distance
from home, is associated with loss of personal
identity and amnesia. There may be a triggering
event such as financial or marital problems.
Recovery of normal learning and alertness is
often sudden, but loss of personal identity and
profound retrograde amnesia may persist, unlike
the usual temporal memory gradient and gradual
recovery seen in organic amnesias. Inability to
recognize their spouse or partner is also
typical. The retrospective forgetting of
circumscribed periods from the past is often
found after distressing events, as in wartime,
but may include periods of alleged criminal
activity in malingerers. Feigned amnesia may be
detected by the 'two-choice' recognition test of
memory, in which malingerers will score
significantly worse than they would by chance.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.